A Brief History Of Marijuana
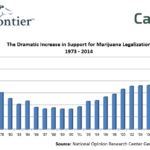
Dramatic Increase In Support For Marijuana Legalization In The U.S. From 1973 To 2014
July 6, 2015
Overview of the Plant
Marijuana is the Mexican colloquial name for the plant genus Cannabis which includes three species, Cannabis Sativa, Cannabis Indica, and Cannabis Ruderalis. Widely believed to have originated in central Asia, cannabis has been cultivated for at least 5,000 years, making it one of mankind’s oldest agricultural commodities.
The plant has long been used for its fibers, its nutritionally rich seeds, and for therapeutic oils. The psychoactive properties of the plant have been used medicinally, recreationally, and religiously by cultures across the globe for millennia.
There are over 400 compounds within the cannabis plant. Of those, over 60 compounds, called cannabinoids, are unique to the plant. The two most notable cannabinoids are:
- Delta 9 Tetrahydrocannabidiol (THC): THC, which is responsible for the psychoactive effects of marijuana, produces the “high” that cannabis users feel. THC is believed to be responsible for some of the powerful curative properties of marijuana such as the anti-emetic and anti-nausea effects.
- Cannabidiol (CBD): These cannabinoids also have potent therapeutic properties but do not have the psychoactive effects of THC. The lack of a mind-altering effect in CBD is why some jurisdictions have limited marijuana access to low-THC/high-CBD strains only.
Cannabis in America: A Winding Journey
The history of cannabis is the United States is a long and complex one. However, understanding the factors that led to its current place in American society is critical to understanding its current perceptions and use, and how the industry is likely to evolve in the future.
The earliest U.S. law on cannabis was passed in 1619 by the Virginia Assembly which required every farmer to grow hemp. The plant was prized in early America for its hardiness—cannabis is highly adaptable and thrives in a wide range of conditions—and the quality of its fibers which were critical to make sails, rigging and other products for the maritime economy.
The plant flourished as the country grew, spreading south where it became a major agricultural commodity, mainly in southern states like Kentucky, Mississippi and Georgia. However, by the mid-19th century, competition from Russia’s cotton and hemp imports had begun to erode demand for domestically grown hemp.
In the years after the U.S. Civil War, the use of cannabis for medicinal purposes began to take off. It became a popular ingredient in medicines to treat migraines, arthritis and insomnia, and was sold both as packages of the marijuana flower and as tinctures.
The plant was primarily used for medicinal purposes until early in the 20th century when Mexican immigrants who were fleeing the Mexican Civil War introduced the practice of smoking it recreationally.
In the 1910’s as the prohibitionist movement gained momentum states began to ban the use of cannabis despite the low prevalence of its recreational use. By 1920 nine states had banned its use, including Massachusetts, Maine, Vermont, Colorado and Nevada.
Despite these restrictions on recreational use, the medicinal use of cannabis continued to grow. By the 1930s, pharmaceutical companies were selling standardized cannabis extracts to treat pain, spasms, and insomnia, and cannabis cigarettes were being touted as treatments for asthma.
However, it wasn’t in the 1930s that momentum against cannabis began to build in earnest. Opponents began calling it marijuana—the Mexican colloquialism—to disassociate it from cannabis and hemp, which were still popular and widely used. And in 1930 the Federal Bureau of Narcotics was formed to coordinate the government’s drug control efforts.
The agency, which was led by Harry J. Anslinger, based its anti-marijuana campaign on two key assertions: marijuana caused insanity, and its use drove people to abhorrent criminal acts. These assertions were effectively captured in the film Reefer Madness, a cautionary tale that showed the irresponsibility and criminality caused by marijuana use.
In 1937, as the threat posed by marijuana captured the public’s imagination, Congress proposed the Marihuana Tax Act which maintained the use of marijuana for medical use only, and required doctors who prescribed it to first register with the federal government and pay an annual tax. The extra steps required to prescribe the drug led many doctors to opt for other, more convenient treatments such as aspirin and morphine, two drugs that were gaining popularity at the time. In 1942, marijuana was removed from the U.S. Pharmacopeia, which ended its legal use as a medicine.
In the 1950s, a succession of laws increased prosecution of marijuana use. The 1951 Boggs Act established two to five year minimum sentences for first time marijuana offenders, including those charged with simple possession, and the inclusion of marijuana in the 1956 Narcotics Control Act further increased the sentencing minimums to two to 10 years, with a fine up to $20,000.
In 1970, Congress passed the Controlled Substance Act which created a five-tier classification system for narcotic and psychotropic drugs. Marijuana was included as a Schedule 1 drug, meaning it had a high potential for abuse and had no currently acceptable medical use.
The classification of marijuana as a Schedule 1 drug was enforced despite the finding by the National Commission on Marijuana and Drug Abuse that “there was little proven danger of physical or psychological harm from the experimental or intermittent use “of marijuana. The Commission went on to recommend that the U.S. adopt a “social control policy seeking to discourage marijuana use, while concentrating primarily on the prevention of heavy and very heavy use,” an approach that favored decriminalization and education over the harsher penalties preferred by prohibitionists.
The Commission’s conclusions, which were based on more than 50 studies it conducted across the U.S. on the perceptions, use, and effects of marijuana, were ultimately rejected by the Nixon administration and in 1971, Nixon declared that “America’s public enemy number one … is drug abuse,” launching the War on Drugs.
Even as the federal government’s enforcement actions gained momentum, propelled by the formation of the Drug Enforcement Agency in 1973, there was a growing movement to harness marijuana’s medical properties at the federal and state level.
In 1976, a judge ruled in favor of Robert Randall, a glaucoma patient in the District of Columbia who had been charged with criminal cultivation of marijuana, citing Randall’s marijuana use as a “medical necessity.” Randall then successfully petitioned the government to provide him FDA-approved medical marijuana, becoming the first American to receive marijuana from the U.S. government to treat a medical condition. The Investigational New Drug Applications, which at its peak provided federally grown marijuana to 30 patients, was ultimately suspended in 1991, as it was perceived to undercut the Bush Administration’s anti-drug policy.
In 1978, New Mexico passed the Controlled Substances Therapeutic Act making it the first state to officially focus on the medical value of marijuana. In 1983, the state released a report on research conducted on cancer patients, concluding that marijuana “is effective as an anti-emetic in treating the effects of chemotherapy (i.e., nausea and vomiting) and additionally, other concomitant symptoms, of both the disease and the therapy (i.e., pain and depression).” Notably, the state found that ingesting a synthetic version of THC was not as effective as smoking the plant.
The growing support for the medical use of marijuana culminated in 1996 when California became the first state in the nation to legalize medical marijuana. The following year, the New England Journal of Medicine published an editorial calling for marijuana to be rescheduled, to which the National Institutes of Health responded by saying further research was first required to assess marijuana’s therapeutic potential before the federal government could recommend rescheduling the plant.
Despite federal opposition to the expansion of state-level medical marijuana laws, four more states—Alaska, Oregon, Washington and Maine—legalized its medical use by 1999.
Two Supreme Court rulings, one in 2001 and one in 2005, challenged California’s medical marijuana laws. In the first case, US vs. Oakland Cannabis Buyers’ Cooperative et al., the court held that there is no medical necessity exception to the Controlled Substances Act’s prohibition on manufacturing and distributing marijuana. In essence, the court ruled that patients could not violate the CSA even if they believed cannabis could treat their conditions. In the second case, Gonzales, Attorney General, et al. v. Raich et al, the court ruled that Congress, through its authority granted by the commerce clause, had “the power to prohibit the local cultivation and use of marijuana” even if the cultivation and use was in compliance with state law.
Despite these rulings, 12 states including Vermont, Rhode Island and New Mexico had approved medical marijuana by 2007, and in 2008 the American College of Physicians (ACP) came out in support of the reclassification of marijuana to allow more research into its medical value. The ACP also recommended the use of non-smoked forms of medical marijuana for conditions where it had been shown to be effective.
In 2009, in a major shift in federal enforcement, the Department of Justice issued the Ogden memo which stated that the agency would not target individuals or businesses that provide or use marijuana in clear compliance with their state’s medical marijuana laws. The same year, the American Medical Association, which had long opposed the use medical marijuana, recommended that “marijuana’s status as a federal Schedule 1 controlled substance be reviewed with the goal of facilitating the conduct of clinical research and development of cannabinoid-based medicines.”
2012 was a watershed year for marijuana policy, as both Colorado and Washington fully legalized the sale, possession and use of marijuana for adults, further highlighting the significant disconnect between federal and state laws. In response, the Department of Justice updated its federal marijuana enforcement policy stating that it would not challenge state marijuana policies but would instead focus on eight priorities related to marijuana, including: preventing distribution of marijuana to minors; preventing diversion of marijuana revenues to gangs and cartels; and preventing drugged driving and other adverse public health consequences.
Even as state laws have quickly evolved, all the lawsuits challenging the federal classification of marijuana as a Schedule 1 drug have failed, including the 2013 case of Americans for Safe Access v. Drug Enforcement Administration in which the U.S. Court of Appeals for the District of Columbia ruled that there were no “adequate and well controlled studies proving efficacy” of marijuana as a medical treatment. The court concluded that the DEA could defer the rescheduling of marijuana until its medical effectiveness has been clinically proven.
Undeterred by the court rulings, more states continued to adopt medical marijuana programs. By 2016, four states and the District of Columbia had legalized full adult use of marijuana, 24 states allowed its medical use, and an additional 11 states had approved the therapeutic use of low-THC/high-CBD products. Support for these state programs was bolstered when Congress passed a law in December 2014 barring the Department of Justice from using funds to enforce the federal ban on marijuana in states which have legalized used of the plant.
Looking Ahead
The wide gulf between federal and state laws is putting the U.S. in an unsustainable position where strong federal prohibition is countered by state-level commercialization of the plant. Furthermore, with at least seven states strongly positioned to legalize full adult use and medical marijuana by 2016, pressure to reconcile federal law with the burgeoning legal state markets will necessarily lead to a shift in federal policy.
While full national legalization remains unlikely in the near term, the passage of a federal marijuana bill, similar to the one currently winding its way through Congress, may be one way for Congress to allow greater exploration and use of medical marijuana without sanctioning its recreational use. However, given the highly contentious current political climate, the likelihood of a bill becoming law before the 2016 presidential elections remains highly uncertain.
With full federal legalization still on the distant horizon, the U.S. will remain a patchwork of widely varied state laws. Due to the prohibition on interstate commerce, businesses seeking to operate in multiple states will face the expense and effort of establishing stand-alone operations and adapting to the variability in each state’s laws. This greatly adds to the costs of expansion for those seeking to enter new markets, but it also creates opportunities for franchising, licensing, and other expansion strategies.

{kind=link}
{kind=link}
{kind=link}